
Symptoms
Anxiety, weakness, tremor, palpitations, sweating, heat intolerance, weight loss, atrial fibrillation, menstrual disorders, osteoporosis
Initial Diagnosis

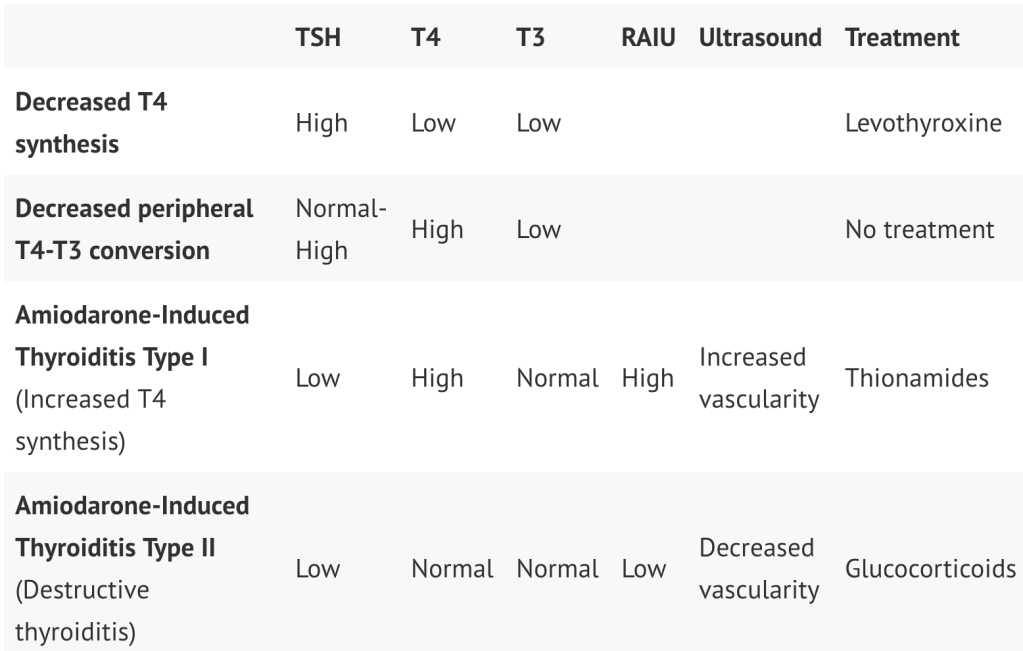
It’s important to also note that Amiodarone may have a variety of effects on thyroid function.
Work-Up/Differential Diagnosis
- High TSH
- Pituitary MRI to look for TSH-secreting pituitary adenoma
- Low TSH
- Positive Thyrotropin-receptor Antibodies
- Graves’ Disease
- Negative Thyrotropin-receptor Antibodies
- Radioactive Iodine Uptake scan (RAIU): tests for uptake of iodine within the thyroid
- High, diffuse uptake
- Points toward Graves’ Disease or pituitary adenoma, however these should have been ruled out earlier in the work-up algorithm.
- Hyperemesis gravidarum (increased nausea and vomiting with pregnancy are associated with an elevated beta-hCG level, which has thyrotropic effects(1))
- Early Hashimoto’s disease
- High, nodular uptake
- Toxic Adenoma
- Toxic Multinodular Goiter (TMNG)
- Low uptake
- Thyroiditis
- Subacute Granulomatous (formerly De Quervain’s) thyroiditis
- Diffuse, firm, tender goiter – generally after viral illness
- Postpartum thyroiditis
- Radiation thyroiditis
- Subacute Granulomatous (formerly De Quervain’s) thyroiditis
- Ectopic production of thyroid hormone
- Struma ovarii
- Teratoma tumor which may contain thyroidal tissue
- Metastatic follicular thyroid cancer
- Struma ovarii
- Exogenous Consumption of thyroid hormone
- Thyroiditis
- High, diffuse uptake
- Radioactive Iodine Uptake scan (RAIU): tests for uptake of iodine within the thyroid
- Positive Thyrotropin-receptor Antibodies
Treatment
- Management of Thyrotoxicosis (“Thyroid Storm”) is discussed separately. General management of thyroiditis will include beta-blockers for symptom control in addition to steroids, however, treatment may differ depending on the etiology. Otherwise, nodules and tumors will require surgical removal (if giving the patient compressive symptoms) or radioactive iodine ablation.
- Graves’ Disease
- Beta-Blockers for hyperthyroid symptoms
- Propranolol
- Antithyroid medication (Thionamides)
- Propylthiouracil (PTU)
- Use in 1st trimester of pregnant patients
- Methimazole
- Use in 2nd/3rd trimesters of pregnant patients
- Propylthiouracil (PTU)
- Thyroidectomy is the preferred definitive treatment.
- Notable risks include recurrent laryngeal nerve laceration, hypocalcemia secondary to inadvertent concomitant parathyroidectomy, bleeding, infection, etc.
- If not a good surgical candidate or if the patient does not want surgery, radioactive iodine ablation of the thyroid is the next best treatment
- Of note, patient must self-isolate for the 1 week after treatment to prevent the risk of spreading radioactivity to others
- Beta-Blockers for hyperthyroid symptoms
References
- T. M. Goodwin, M. Montoro, and J. H. Mestman, “The role of chorionic gonadotropin in transient hyperthyroidism of hyperemesis gravidarum,” Journal of Clinical Endocrinology and Metabolism, vol. 75, no. 5, pp. 1333–1337, 1992.
