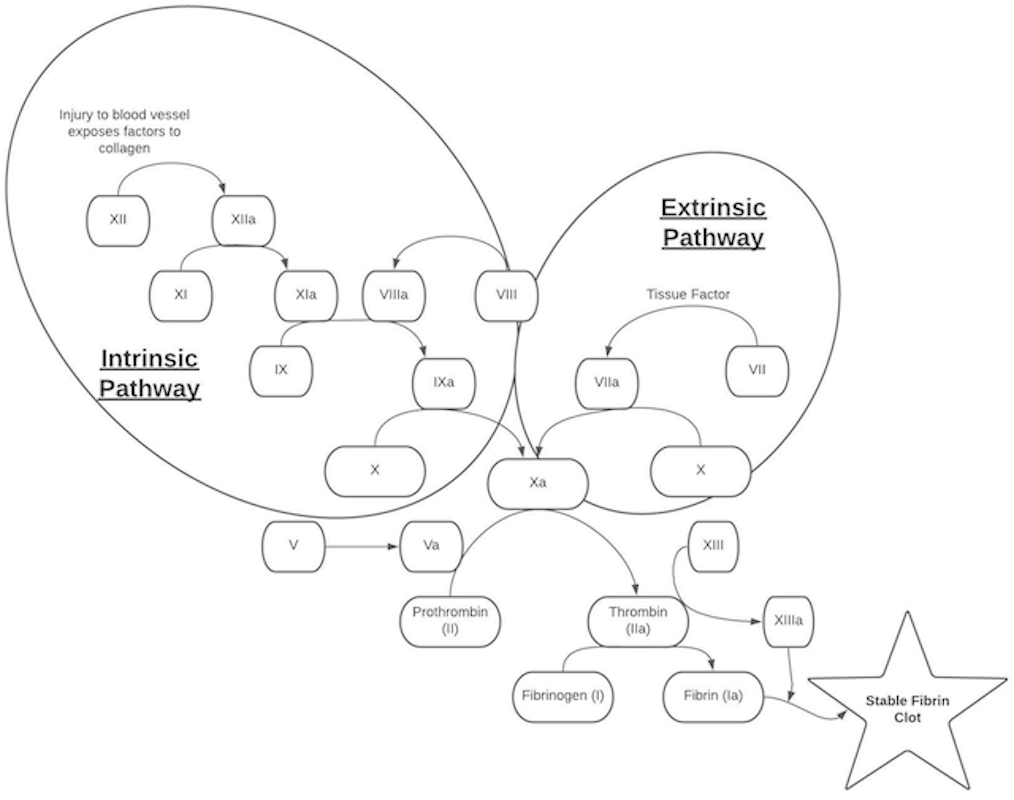
Coagulation Cascade
Coagulation Labs
PT (Prothrombin Time): Thromboplastin (which contains Tissue Factor) is added to blood and the time needed to clot is recorded. Specifically analyzes the extrinsic pathway (factors II, V, VII, and X, and fibrinogen) (1)
INR (International Normalized Ratio): Because of variability in thromboplastin reagent mixtures around the world, the INR was developed to give a standardized number based on a ratio of the patient’s PT divided by a control PT using an internationally-accepted thromboplastin reagent. (1)
PTT (Partial Thromboplastin Time) aka aPTT (activated Partial Thromboplastin Time): Kaolin is added to a sample of the patient’s blood, which leads to activation of the intrinsic coagulation pathway. This test measures, collectively, all factors except VII and XIII (2)
Anticoagulants
Warfarin inhibits Vitamin K Epoxide Reductase Complex (VKORC), which inhibits this enzyme’s ability to recycle Vitamin K. This leads to a decrease in the number of Vitamin-K dependent coagulation factors, which are Factors II, VII, IX, X, and Proteins C and S. This prolongs the PT (in turn increasing the INR) and PTT
Heparin forms a complex with antithrombin III, which then inactivates thrombin and Factors IXa, Xa, and XIa. This prolongs the PTT, although many low-molecular weight heparins (such as enoxaparin) will not prolong the PT. Heparin should also, in theory, prolong the PT (in turn increasing the INR), however, most PT reagents contain heparin-binders, which remove heparin from the equation, allowing for a normal PT reading (3)
DOACs (Direct Oral Anticoagulants)
- Direct Thrombin Inhibitors: Dabigatran, argatroban, bivalirudin
- Factor Xa Inhibitors: Apixaban, rivaroxaban, edoxaban, betrixaban, fondaparinux
These agents may prolong the PT (and increase the INR) as well as prolong the PTT; however, patients who are anticoagulated therapeutically on these agents may still have normal studies. Therefore, routine monitoring of these labs is not recommended (4, 5, 6)
Bleeding Disorders
Hemophilia A: Factor VIII deficiency (7)
- Inheritance: X-linked recessive
- PT/INR: normal, PTT: generally prolonged
- Diagnosis: Serum factor VIII levels
- Management: Depends on severity of disease. Desmopressin can stimulate endothelial cells to secrete Von Willebrand factor (VWF) which protects the limited amount of Factor VIII in the body
Hemophilia B (Factor IX deficiency) (8)
- Inheritance: X-linked recessive
- PT/INR: normal, PTT: generally prolonged
- Diagnosis: Serum factor IX levels
- Management: Recombinant factor IX prophylactically dosed twice per week or at a higher dose in acute bleeding events. Antifibrinolytic agents (Monoclonal antibodies (e.g., rituximab), tranexamic acid, and epsilon aminocaproic acid) can be used in cases of mucosal bleeding or dental extractions
Vitamin K Deficiency/Liver Disease
- Vitamin K deficits generally as a result of reduced dietary intake (or reduced absorption due to a biliary obstruction), diarrhea, or antibiotic use
- Vitamin K deficiency results in decreased synthesis of factors II, VII, IX, X, and proteins C and S. Liver disease results in decrease in production of all coagulation factors (except factor VIII)
- PT/INR: Elevated, PTT: Elevated
- Diagnosis: PT/INR, PTT, evidence of liver disease on routine laboratory studies (CMP)
- Management: PO or IV Vitamin K replacement; may also use fresh frozen plasma (FFP)
Von Willebrand Disease (VWD) (9)
- 3 sub-types
- Type 1 (Autosomal Dominant) (most common): Deficiency of VWF
- Type 2: (Autosomal Dominant) Abnormal, decreased functioning of VWF
- Type 3: (Autosomal Recessive) Total or near-total absence of VWF
- PT/INR: normal, PTT: normal or elevated depending on severity of the disease (because of the subsequent deficiency of Factor VIII caused by low levels of VWF)
- Diagnosis: VWF Factor Antigen levels and VWF Factor Activity levels
- Management: DDAVP in minor bleeding episodes (generally only useful in Type 1 and Type 3). VWF can be replaced in major bleeding episodes that do not demonstrate a response to DDAVP.
Clotting Disorders
Factor V Leiden mutation (10)
- Most common inherited thrombophilia
- Mechanism: Point mutation in Factor V and Va prevents activated Protein C (aPC) from cleaving them, leading to increased thromboembolism risk
- Diagnosis: Mutation testing or Functional aPC resistance assays
- Management: Anticoagulation if the patient has a VTE, recommended for the same indications and duration as VTE in the general population
Antiphospholipid Antibody Syndrome (11)
- Autoantibodies against phospholipids and phospholipid-binding proteins, such as cardiolipin and β2-glycoprotein I.
- Can be primary/idiopathic, or may be secondary to underlying autoimmune diseases, malignancy, or drugs
- Diagnosis:
- Lupus anticoagulant: measures the effect that the antibody has on clotting time. Antiphospholipid antibodies bind to phospholipids in the blood sample, preventing clotting. The name is somewhat paradoxical – blood is prevented from clotting in the test tube, but at a higher risk of clotting in vivo.
- Anticardiolipin antibody
- Anti-Beta-2-glycoprotein-I antibody
- Treatment: Anticoagulation
Antithrombin III Deficiency (12)
- Antithrombin III normally functions to inhibit thrombin as well as factors Xa, IXa, and VIIa. Inherited or may be acquired in liver disease, nephrotic syndrome, DIC, sepsis, pre-eclampsia
- Type I: Quantitative defect
- Type II: Qualitative defect
- Diagnosis: Antithrombin III levels
- Management:
- Anticoagulation for patients with a VTE. Prophylactic anticoagulation for pregnant women or patients who are to undergo surgery
- Low-molecular weight heparin generally preferred, followed by warfarin or DOACs
- Antithrombin III concentrate may be useful in patients with recurrent VTE despite anticoagulation, heparin-resistance, or patients on ECMO or hemodialysis
Protein C Deficiency (13)
- Protein C is vitamin K–dependent, converted into activated Protein C (aPC), which inactivates coagulation factors Va and VIIIa. Deficiency leads to increased risk of coagulation and thrombotic events
- Inheritance: Autosomal Dominant
- Diagnosis: Clotting assays, ELISA, and chromogenic tests to determine levels of protein C activity
- Management: Long-term Protein C replacement or anticoagulation with warfarin or low-molecular weight heparin
Paroxysmal Nocturnal Hemoglobinuria (14)
- Mutation of PIG-A gene, leading to paucity of several surface membrane proteins on RBCs, including CD55 and CD59. This leads to increased complement-mediated lysis of RBCs
- Hypercoagulability attributed mostly to increased complement-mediated activation of platelets
- Diagnosis: Flow cytometry
- Treatment: supportive treatment of hemolysis. Prophylactic anticoagulation remains controversial, however, management of thrombosis secondary to PNH with lifelong anticoagulation is generally accepted
Polycythemia Vera/Essential Thrombocytosis
- Can screen for with CBC
Oral Contraceptive use (15)
- Estrogen/progestins increase plasma fibrinogen levels, coagulation factor activity, and decrease antithrombin III levels, in addition to accelerating platelet aggregation
- Management: Discontinue oral contraceptives
References:
- Yang, R. (2021, May 10). Prothrombin Time. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK544269/.
- Rountree, K. M. (2020, August 21). Partial Thromboplastin Time. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK507772/.
- DM;, F. (n.d.). Coagulation assays and anticoagulant monitoring. Hematology. American Society of Hematology. Education Program. https://pubmed.ncbi.nlm.nih.gov/23233620/.
- Kovacevic MP;Lupi KE;Wong A;Gilmore JF;Malloy R; (n.d.). Evaluation of the Effect of Apixaban on INR in the Inpatient Population. Journal of cardiovascular pharmacology and therapeutics. https://pubmed.ncbi.nlm.nih.gov/30905167/.
- Frans, G., Meeus, P., & Bailleul, E. (2019, June 12). Resolving DOAC interference on aPTT, PT, and lupus anticoagulant testing by the use of activated carbon. Wiley Online Library. https://onlinelibrary.wiley.com/doi/full/10.1111/jth.14488.
- Adcock, D. M., & Gosselin, R. C. (2017, April 26). The danger of relying on the APTT and PT in patients on DOAC therapy, a potential patient safety issue. Wiley Online Library. https://onlinelibrary.wiley.com/doi/full/10.1111/ijlh.12658.
- Centers for Disease Control and Prevention. (2020, July 17). Diagnosis of Hemophilia. Centers for Disease Control and Prevention. https://www.cdc.gov/ncbddd/hemophilia/diagnosis.html.
- Alshaikhli, A. (2021, February 6). Hemophilia B. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK560792/.
- Sabih, A. (2021, March 6). Von Willebrand Disease. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK459222/.
- Albagoush, S. A. (2021, March 1). Factor V Leiden Deficiency. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK534802/.
- Mezhov, V., Segan, J. D., Tran, H., & Cicuttini, F. M. (2019, July 4). Antiphospholipid syndrome: a clinical review. Wiley Online Library. https://onlinelibrary.wiley.com/doi/10.5694/mja2.50262.
- Găman, A. M., & Găman, G. D. (2014). Deficiency Of Antithrombin III (AT III) – Case Report and Review of the Literature. Current health sciences journal. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4340457/.
- Gupta, A. (2021, January 29). Protein C Deficiency. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK542222/.
- Risitano, A. M., & Rotoli, B. (2008, June). Paroxysmal nocturnal hemoglobinuria: Pathophysiology, natural history and treatment options in the era of Biological Agents. Biologics : targets & therapy. Retrieved November 17, 2021, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2721357/.
- J;, B. (n.d.). Coagulation effects of oral contraception. American journal of obstetrics and gynecology. Retrieved November 17, 2021, from https://pubmed.ncbi.nlm.nih.gov/2960241/.
