
Starters
- Potassium is largely an intracellular electrolyte
- Intracellular potassium is regulated through the Na+/K+ ATPase channel
- Normal serum K+ levels: 3.5 – 5.0 mEq/L
- Consider repeating lab draw: False hyperkalemic readings may results from drawing from an IV with a potassium-rich fluid running through it. Also, prolonged tourniquet constriction of arm during blood draw can cause localized cell lysis and false readings of hyperkalemia
Etiologies
- High intake
- Lactated Ringer’s
- Penicillin G
- Total parenteral nutrition (TPN)
- Low output (90% of serum K+ is excreted through the kidney 1)
- Acute Kidney Injury (AKI)
- Type 4 Renal Tubular Acidosis (Hypoaldosteronism)
- Medications (Most of these share the end effect of decreasing the level of aldosterone in the body)
- ACE Inhibitors (ACEI): Lisinopril, captopril, etc.
- Angiotensin-Receptor Blockers (ARBs): Losartan, valsartan, etc.
- Aldosterone-Receptor Antagonists: Spironolactone, eplerenone
- Epithelial Na+ channel (ENaC) inhibitors: Amiloride, triamterene
- NSAIDs
- Ketoconazole (inhibits aldosterone synthase)
- K+ shifting from intracellular to extracellular
- Acidemia: Stimulates H+/K+ exchange channels, shifting H+ inside the cell and K+ out of the cell
- Hypertonicity: Causes water to flow out of cell, potassium moves with it
- Cell Lysis
- Tumor Lysis Syndrome
- Rhabdomyolysis
- Trauma
- Hemolysis
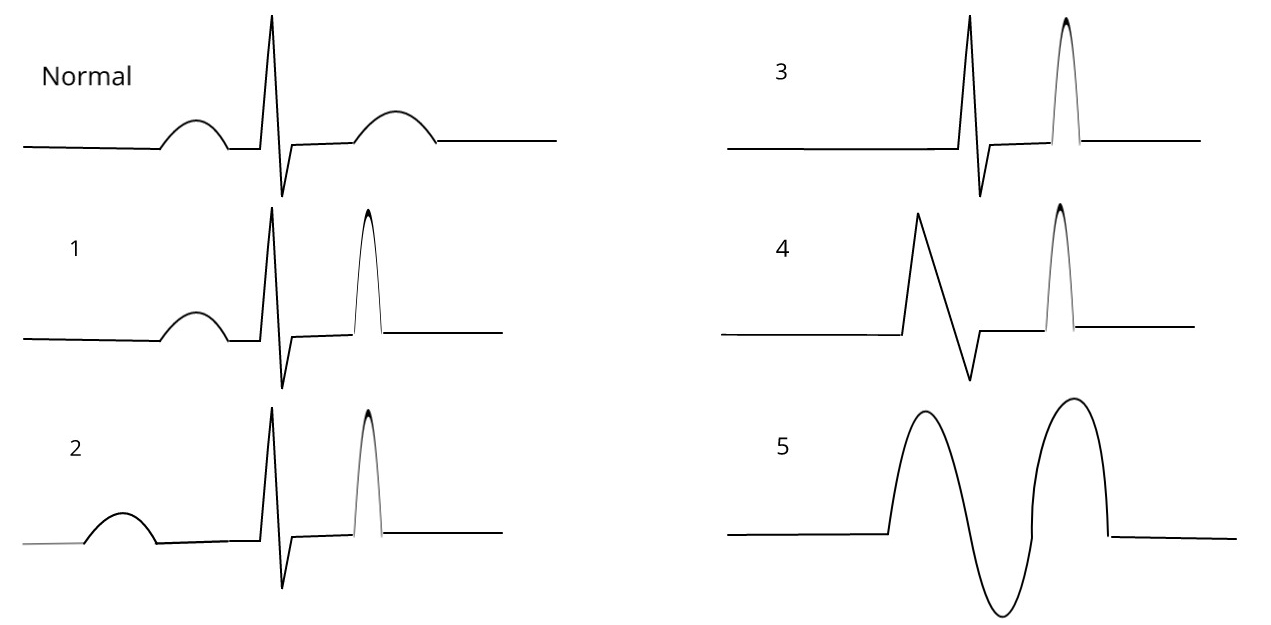
EKG changes
- 1st: “Peaked” T-waves
- 2nd: Prolonged PR interval
- 3rd: Loss of P-waves
- 4th: Prolonged QRS interval
- 5th: Sinusoidal waves
- 6th: Ventricular arrhythmia
Management
- Stabilize the cardiac membrane
- Calcium gluconate
- Indications: Conduction abnormalities on EKG or significantly elevated potassium level (generally > 6.5 mEq/L)
- Physiology: The Nernst equation tells us that in hyperkalemia, the resting membrane potential is shifted to a less negative value. Therefore, a lower stimulation is necessary to generate an action potential. However, after repeated depolarizations, sodium channels in the membrane become inactivated. This leads to a decreased ability of the cardiac muscle to generate action potentials (2). Administration of calcium shifts the threshold potential of the membrane to a less negative value, so that the difference between the resting membrane potential and the threshold potential remains ~15 mV (3)
- Effect lasts ~30 minutes, so repeated administration is necessary if still indicated
- Calcium gluconate
- Decrease serum potassium levels
- Quick, temporary
- IV Regular Insulin
- Stimulates Na+/K+ ATPase
- Give D50W at the same time to avoid hypoglycemia
- IV Sodium Bicarbonate
- Increases serum pH, causing cell membrane H+/K+ exchange channels to activate, shifting H+ outside the cell and K+ into the cell
- β-2 agonist (e.g. albuterol)
- Stimulates Na+/K+ ATPase
- IV Regular Insulin
- Slow, permanent
- Loop diuretics (e.g. furosemide)
- Increase renal excretion of potassium
- Sodium polystyrene
- Increases GI excretion of potassium (but, as above, ~90% of potassium is excreted through kidneys)
- Loop diuretics (e.g. furosemide)
- Quick, temporary
- Dialysis
- Indicated if:
- Symptomatic (weakness/paralysis)
- Conduction abnormalities on EKG
- Hyperkalemia refractory to above therapies
- Severe renal dysfunction
- Significantly elevated potassium level (generally > 6.5 mEq/L)
- Indicated if:
References
- Nohara‐Shitama, Y., Yume Nohara‐Shitama Division of Cardio‐Vascular Medicine, Adachi, H., Hisashi Adachi Division of Cardio‐Vascular Medicine, Enomoto, M., Mika Enomoto Division of Cardio‐Vascular Medicine, . . . Adachi, *. (2018, January 04). Twenty‐four‐Hour Urinary Potassium Excretion, But Not Sodium Excretion, Is Associated With All‐Cause Mortality in a General Population. Retrieved January 12, 2021, from https://www.ahajournals.org/doi/full/10.1161/jaha.117.007369
- RM, B., & MN, L. (1981). Cardiovascular Physiology, 4th edition. St. Louis, MO: Mosby.
- Parham, W., Mehdirad, A., Biermann, K., & Fredman, C. (2006). Hyperkalemia revisited. Retrieved January 12, 2021, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1413606/
